
|
|
Beta Blockers No More First Choice for Hypertension
Jun 29, 2006, 01:18, Reviewed by: Dr. Sanjukta Acharya
|
|
The decision not to recommend Beta-blockers for first line therapy is based on evidence that suggests that they perform less well than other drugs, particularly in the elderly, and the increasing evidence that the most frequently used Beta-blockers at usual doses carries an unacceptable risk of provoking type 2 diabetes.
|
By M.I.N.D.S.,
The National Institute for Health and Clinical Excellence (NICE), UK and the National Collaborating Centre for Chronic Conditions, in conjunction with the British Hypertension Society (BHS) on Wednesday 28 June launched the keenly awaited updated clinical guideline on the management of hypertension. The guideline updates the recommendations for the pharmacological management of hypertension contained in the original NICE guideline published in August 2004. Based on a thorough review of recently published data, the guideline sets the gold standard for the optimum pharmacological management of hypertension and in so doing seeks to decrease morbidity and mortality resulting from cardiovascular diseases such as stroke, chronic renal failure and coronary heart disease for which hypertension is a significant risk factor.
It is estimated that some 40 per cent of adults in England and Wales have hypertension and this proportion increases with age. In 2001, the NHS funded 90 million prescriptions for drugs that lower blood pressure, accounting for nearly 15 per cent of the total annual cost of all primary care drugs. Nonetheless, hypertension is often inadequately treated.
In formulating the recommendations, the Guideline Development Group (GDG) considered not only data from the new studies, but also adverse events data and a detailed health economic analysis comparing the cost-effectiveness of the main drug classes. The GDG also considered the cause, development, and effects of hypertension and the mechanism of action of the different classes of blood pressure lowering drugs allowing for age and ethnicity.
 |
| Courtesy: Blood Pressure Association (BPA) |
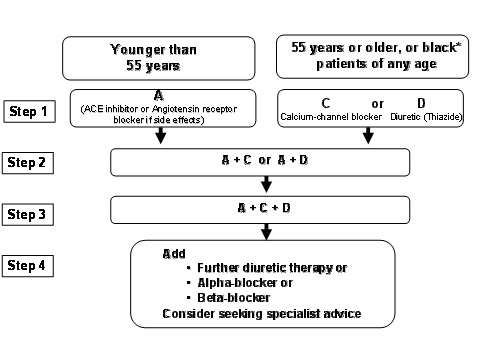
The updated recommendations in the guideline include the following:
� In hypertensive patients aged 55 and over, or Black patients* of any age, first choice of initial therapy should be either a calcium channel blocker or a thiazide-type diuretic.
*Black patients are those of African or Caribbean descent, and not mixed race, Asian or Chinese patients.
� In hypertensive patients younger than 55, first choice initial therapy should be an ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated).
� If initial therapy was with a calcium channel blocker or thiazide-type diuretic and a second drug is required, add an ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated). If initial therapy was with an ACE inhibitor, add a calcium channel blocker or a thiazide-type diuretic.
� If treatment with three drugs is required, the combination of ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated), calcium channel blocker and thiazide-type diuretic should be used.
The decision not to recommend Beta-blockers for first line therapy is based on evidence that suggests that they perform less well than other drugs, particularly in the elderly, and the increasing evidence that the most frequently used Beta-blockers at usual doses carries an unacceptable risk of provoking type 2 diabetes. The guideline also makes recommendations beyond a 3-drug combination, where, although the evidence is less certain, the GDG took into account existing guidelines and constructed recommendations most compatible with current good practice.

- National Institute for Health and Clinical Excellence (NICE)
www.nice.org.uk/CG034guidance
The National Institute for Health and Clinical Excellence (NICE) is the independent organisation responsible for providing national guidance on the promotion of good health and the prevention and treatment of ill health.
NICE produces guidance in three areas of health:
� public health � guidance on the promotion of good health and the prevention of ill health for those working in the NHS, local authorities and the wider public and voluntary sector
� health technologies � guidance on the use of new and existing medicines, treatments and procedures within the NHS
� clinical practice � guidance on the appropriate treatment and care of people with specific diseases and conditions within the NHS.
The British Hypertension Society (BHS) provides a medical and scientific research forum to enable sharing of cutting edge research in order to understand the origin of high blood pressure and improve its treatment. The BHS has a track record of producing internationally renowned guidelines for the management of hypertension which are widely adopted in primary care in the UK and elsewhere. The BHS has also established an educational programme to support scientists, doctors and other healthcare workers involved in understanding the basis of high blood pressure and improving its treatment throughout the UK.
Four versions of the guidance will be available on the NICE website (www.nice.org.uk/CG034) from 28 June 2006:
� the full guideline, Clinical guideline 34: �Hypertension: management of hypertension in adults in primary care: partial update www.nice.org.uk/CG034guidance
� the NICE guideline, �Hypertension: management of hypertension in adults in primary care www.nice.org.uk/CG034NICEguideline
� a �Quick reference guide www.nice.org.uk/CG034quickrefguide (also available from the NHS Response Line � telephone 0845 155 455 and quote reference number N1050)
� information for patients and carers, �Understanding NICE guidance� www.nice.org.uk/CG034publicinfo (also available from the NHS Response Line � quote reference number N1051).
|
For any corrections of factual information, to contact the editors or to send
any medical news or health news press releases, use
feedback form
Top of Page
|
|
|
|