|
From rxpgnews.com Hypertension
The National Institute for Health and Clinical Excellence (NICE), UK and the National Collaborating Centre for Chronic Conditions, in conjunction with the British Hypertension Society (BHS) on Wednesday 28 June launched the keenly awaited updated clinical guideline on the management of hypertension. The guideline updates the recommendations for the pharmacological management of hypertension contained in the original NICE guideline published in August 2004. Based on a thorough review of recently published data, the guideline sets the gold standard for the optimum pharmacological management of hypertension and in so doing seeks to decrease morbidity and mortality resulting from cardiovascular diseases such as stroke, chronic renal failure and coronary heart disease for which hypertension is a significant risk factor.
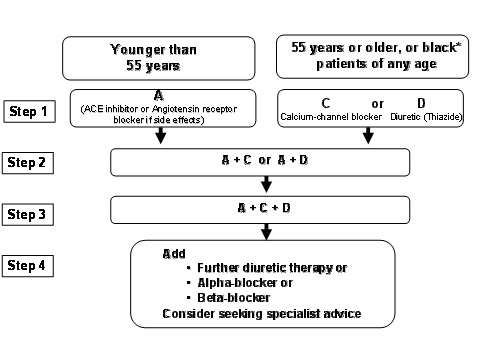
The updated recommendations in the guideline include the following: � In hypertensive patients aged 55 and over, or Black patients* of any age, first choice of initial therapy should be either a calcium channel blocker or a thiazide-type diuretic. *Black patients are those of African or Caribbean descent, and not mixed race, Asian or Chinese patients. � In hypertensive patients younger than 55, first choice initial therapy should be an ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated). � If initial therapy was with a calcium channel blocker or thiazide-type diuretic and a second drug is required, add an ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated). If initial therapy was with an ACE inhibitor, add a calcium channel blocker or a thiazide-type diuretic. � If treatment with three drugs is required, the combination of ACE inhibitor (or an Angiotensin receptor blocker if an ACE inhibitor is not tolerated), calcium channel blocker and thiazide-type diuretic should be used. The decision not to recommend Beta-blockers for first line therapy is based on evidence that suggests that they perform less well than other drugs, particularly in the elderly, and the increasing evidence that the most frequently used Beta-blockers at usual doses carries an unacceptable risk of provoking type 2 diabetes. The guideline also makes recommendations beyond a 3-drug combination, where, although the evidence is less certain, the GDG took into account existing guidelines and constructed recommendations most compatible with current good practice. All rights reserved by www.rxpgnews.com |